Blogs
Mechanical Ventilation – Advance Ventilation Modes
Date: November 29, 2023 | Posted by: Vikram Aditya Tirthani
Date: November 29, 2023 | Posted by: Vikram Aditya Tirthani
In continuation to the earlier topic Mastering Mechanical Ventilation- Basic Ventilation Modes, here is the comprehensive guide for Advanced ventilation modes.
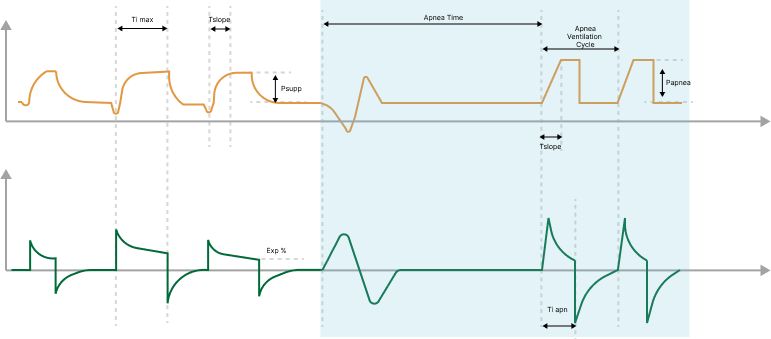
BIPAP or DuoLevel or Bilevel is a ventilation mode that offers two alternating levels of continuous positive airway pressure (CPAP) to support spontaneous breathing. The ventilator automatically switches between these operator-selected CPAP levels at regular intervals, guided by DuoLevel timing settings or patient effort. In this mode, patients have the flexibility to breathe either through mechanical ventilation or spontaneously at the chosen pressure level.
Here’s how it works:
The following figure shows typical waveforms for BiPAP or Dual pressure modes –

This mode can function differently based on settings and the presence of spontaneous breathing. In conventional settings and without spontaneous breathing, it resembles the Pressure Assist/Control (P-A/C) mode. However, as you decrease the rate and keep T high relatively short compared to the time at the lower pressure level, it becomes more similar to Pressure Support Intermittent Mandatory Ventilation (PSIMV), where spontaneous breaths follow mandatory breaths.
APRV is a ventilation mode where airway pressure alternates between two levels: a high pressure (P high) and a lower pressure (P low). It briefly releases to P low before quickly returning to re-inflate the lungs. Importantly, APRV allows for spontaneous breathing at any point in the respiratory cycle, providing flexibility.
In essence, APRV can be thought of as a periodic, short-duration release of airway pressure within a Continuous Positive Airway Pressure (CPAP) framework.
The figure below illustrates typical waveforms in APRV mode, offering a visual representation of how this mode operates.

For patients without spontaneous breathing efforts, APRV resembles the Pressure Control Ventilation (PCV) mode with inverse ratio ventilation.
functions similarly to the conventional volume-controlled mode of ventilation (CMV), with the key difference being that pressure is the control variable rather than flow. In PRVC, breaths can be triggered either by the ventilator or the patient. If the breath is triggered by the patient, the inspiratory rate may increase.
In PRVC, the delivered breaths are volume-targeted and mandatory. They are delivered at the lowest possible pressure while maintaining the desired tidal volume. The gas volume delivered is guaranteed to be equal to the preset tidal volume. The pressure during ventilation will vary according to the set tidal volume and the resistance and compliance of the patient’s lungs.
The ventilator incorporates a safety feature, using the high-pressure alarm limit minus 5 cmH2O as a boundary for inspiratory pressure adjustments, ensuring that it does not exceed this value. An exception to this rule is during sigh breaths, when the ventilator may briefly apply inspiratory pressures 3 cmH2O below the high-pressure alarm limit.
The first PRVC cycle is used for experimental ventilation. The gas delivery pressure during the first cycle is set at 10 cmH2O plus PEEP (Positive End-Expiratory Pressure). This initial setting is used for calculating the compliance and resistance of the entire system, including the patient’s lungs, and for determining the pressure level based on the patient’s condition.
Subsequent breaths are adjusted individually, increasing the delivered volume by modifying the ventilator’s pressure settings. For the first three cycles, the pressure cannot exceed 10 cmH2O, and for the following cycles, it cannot exceed 3 cmH2O. The maximum pressure should not surpass the high-pressure alarm limit minus 5 cmH2O.
The figure below illustrates typical waveforms in APRV mode, offering a visual representation of how this mode operates

Once the pressure level has been adjusted and stabilized, it serves as the reference point for regulating tidal volume in the subsequent ventilation cycles.
PRVC-SIMV stands for Pressure-Regulated Volume Control – Synchronized Intermittent Mandatory Ventilation, offers a mix of features from PRVC, SIMV, and SPONT modes. It delivers two types of breaths: volume-targeted mandatory breaths and pressure-supported spontaneous (patient-triggered) breaths.
This mode ensures that the preset target volume is delivered in the minimum number of mandatory breaths based on the intermittent mandatory ventilation frequency.
If a patient triggers a breath within a 5-second trigger window (1.5 seconds for pediatrics and neonates), the ventilator delivers one mandatory volume-controlled breath. If no trigger occurs by the end of the trigger window, the ventilator also delivers one mandatory PRVC breath. Outside the trigger window, spontaneous or pressure-supported breathing is supported. If the patient doesn’t trigger a breath during the entire expiratory phase, the ventilator automatically delivers a mandatory breath at the end of the expiratory cycle.
The following figure shows typical waveforms in PRVC-SIMV mode –

To ensure safety, the ventilator maintains inspiratory pressure adjustments within the high-pressure limit minus 5 cmH2O, with an exception for sigh breaths, where the ventilator may apply inspiratory pressures 3 cmH2O below the high-pressure limit.
nCPAP is nasal continuous positive airway pressure ventilation mode. The nCPAP mode is available only in NIV and is supposed to be used only with neonatal patients.
In this mode, the airway pressure is held at the user-set positive pressure level throughout the ventilation cycle. The patient breathes spontaneously and determines his own breathing frequency, tidal volume, and breath time.
The following figure shows typical waveforms in nCPAP mode

These modes adjust the patient’s ventilation parameters based on minimum work of breathing (WOB). the user only needs to enter the patient’s ideal body weight (IBW) and target minute ventilation volume percentage, the ventilator will calculate the tidal volume and breathing frequency with the minimum WOB using the Otis equation. It will also adjust the I:E ratio depending on the measured lung time constant. Otis’s equation on which parameters are calculated is as below –

Where f is the breathing frequency under minimum WOB, MV is the target minute volume, Vd is the volume of the patient’s physiological dead space, RCexp refers to the time constant of the lung, a is coefficient of the waveform, For sine-wave,
a=2π2/60
The first few cycles of these modes of experimental ventilation to calculate the patient’s lung resistance and compliance.
After these experimental breaths, enter the automatic adjustment stage. Based on the principle of minimum WOB, ensure that the actual minute volume is as close as possible to the target minute volume value. Mandatory ventilation is administered if the patient has no spontaneous breathing. Support ventilation is administered if the patient restores spontaneous breathing.
Target minute volume is calculated by multiplication combinations these combinations when placed in a graph, generate the ideal curve.
High-flow oxygen therapy is a method to raise the oxygen concentration in the airway at normal pressure through simple tube connections. It increases the oxygen concentration in the alveolar gas, facilitating oxygen diffusion to boost PaO2 and SpO2 saturation. This helps alleviate or correct hypoxia by increasing the oxygen concentration in the inhaled air. Oxygen therapy is a means of preventing or treating hypoxia by providing oxygen concentrations higher than those in the surrounding air.
It is a respiratory support method in which a patient who is breathing on his own, is provided heated, humidified oxygen or air. The flow rate, typically between 2 and 80 liters per minute, can exceed the patient’s inhalation rate, ensuring a comfortable and humidified high oxygen supply.
This therapy is often administered through a nasal cannula or similar interfaces and can provide oxygen concentrations of up to 100%. High-flow oxygen therapy is used to support oxygenation in various medical situations, with precise control of temperature and humidity to match or exceed the patient’s breathing rate.
Get in touch with us using our contact form.