Blogs
Optimizing Ventilator Management for Pulmonary Dead Space
Date: November 29, 2023 | Posted by: Vikram Aditya Tirthani
Date: November 29, 2023 | Posted by: Vikram Aditya Tirthani
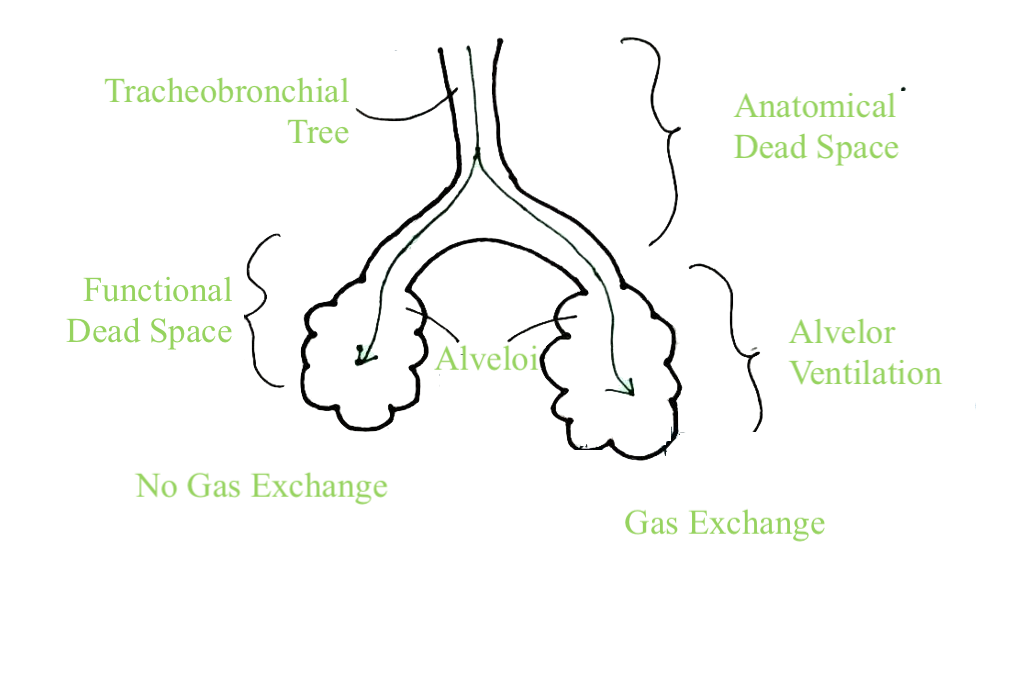
Pulmonary dead space refers to the portion of each breath that does not participate in gas exchange with the blood. It represents the volume of air that ventilates the non-perfused or under-perfused alveoli, where oxygen exchange cannot occur. Understanding dead space is vital for comprehending the efficiency of our respiratory system in delivering oxygen to the body and expelling carbon dioxide.
Anatomical dead space refers to the air contained in the respiratory system’s conducting airways, including the nose, trachea, bronchi, and bronchioles. This volume, although not involved in gas exchange, is necessary for the initial phases of breathing.
Alveolar dead space involves the ventilated alveoli that do not contribute to gas exchange due to factors like impaired blood flow or damage. Conditions such as pulmonary embolism or emphysema can lead to alveolar dead space, limiting the efficiency of oxygen exchange.
Physiological dead space is the combination of anatomical and alveolar dead space. It represents the total volume of gas that does not participate in effective ventilation and perfusion.
Several methods are employed to measure dead space, providing valuable insights into respiratory function:
The Bohr equation calculates physiological dead space using measurements of exhaled carbon dioxide and arterial carbon dioxide levels.
Capnography, a non-invasive method, monitors the concentration of carbon dioxide in exhaled air. Changes in end-tidal carbon dioxide levels can indicate alterations in dead space.
Volumetric methods involve the use of specialized equipment to measure dead space, including nitrogen washout and helium dilution techniques.
Understanding and evaluating pulmonary dead space is crucial in various respiratory scenarios:
Conditions like pulmonary embolism can increase dead space by limiting blood flow to certain areas of the lungs, affecting gas exchange.
In COPD, changes in lung structure and increased anatomical dead space can contribute to inefficient ventilation.
ARDS may lead to an increase in physiological dead space due to alveolar damage and impaired gas exchange
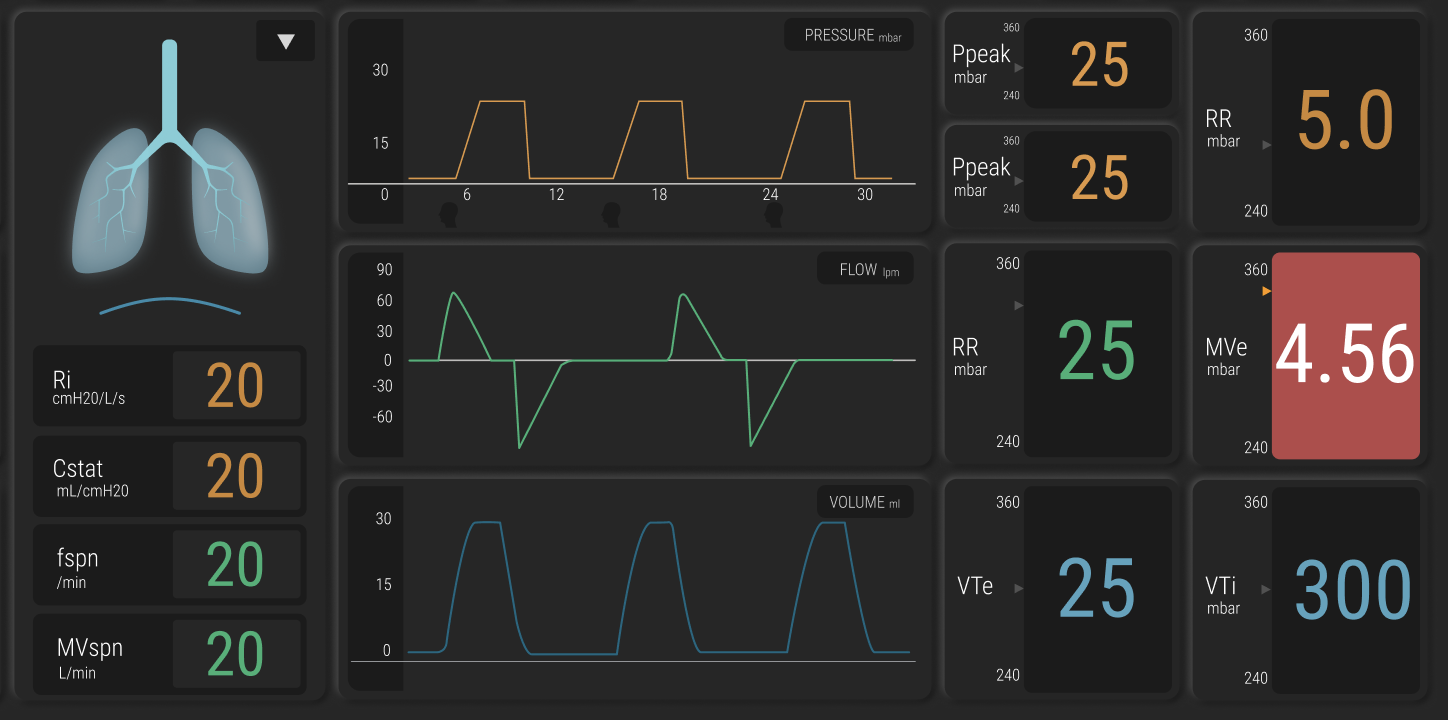
Adjusting tidal volume on the ventilator is a fundamental strategy. It involves setting the volume of air delivered with each breath to ensure effective ventilation without causing unnecessary overdistension of alveoli.
PEEP is a crucial parameter in managing dead space. By maintaining positive pressure in the lungs at the end of expiration, PEEP prevents alveolar collapse, improves oxygenation, and reduces physiological dead space.
Modifying the respiratory rate on the ventilator influences the amount of fresh air brought in and the removal of carbon dioxide. Fine-tuning this parameter helps strike a balance between ventilation and avoiding unnecessary dead space ventilation.
Capnography, measuring end-tidal carbon dioxide levels, is a valuable tool for assessing the efficiency of ventilation. Monitoring changes in capnography waveforms can guide adjustments to ventilation parameters to minimize dead space.
Optimizing inspiratory time helps in maximizing the time available for gas exchange while avoiding unnecessary overdistension. It involves finding the right balance to enhance ventilation efficiency.
Recognizing that each patient’s respiratory dynamics are unique is paramount. Tailoring ventilator settings to the specific needs and conditions of the patient helps in optimizing ventilation and minimizing dead space.
Patient-specific factors, such as lung compliance and airway resistance, vary widely. Ventilator management must consider these individual characteristics to achieve optimal outcomes.
Continuous monitoring of ventilator parameters, along with real-time feedback from capnography and other respiratory assessments, enables clinicians to promptly adjust settings as needed.
Collaborative decision-making involving respiratory therapists, intensivists, and other healthcare professionals ensures a comprehensive and effective approach to managing dead space.
Effectively managing a ventilator for pulmonary dead space requires a dynamic and patient-centric approach. By carefully adjusting tidal volume, utilizing PEEP, monitoring respiratory parameters, and considering individual patient factors, clinicians can enhance ventilation efficiency and minimize the impact of dead space. This multidimensional strategy ensures that ventilator management aligns with the unique respiratory needs of each patient, ultimately optimizing respiratory care and improving patient outcomes.
Get in touch with us using our contact form.